One of most enjoyable aspects of starting this blog has been the feedback that I have received. There was a lot of interest regarding my January post on Marijuana’s impact on Quality of Life (QoL). I want to use this opportunity to continue the conversation that we started almost 6 months ago.
I recently presented a review of all of the research related to Quality of Life and Marijuana use at my hospital’s Psychiatry Grand Rounds. In my previous post, we looked at 3 studies that used validated Quality of Life (QoL) scales to evaluate the associations between Marijuana and QoL. Since then, I have reviewed the 6 additional studies that are currently available. This relatively small number of studies available stands in contrast to 54 articles related to Quality of Life and Cigarette Smoking which are available.
DEA Scheduling Limits Research
Unfortunately, the paucity of research of marijuana and cannabis is not just limited to QoL studies. The shortage of research studies is directly due to the fact that Marijuana remains a DEA Schedule I substance. Because the DEA considers Marijuana to be in the same class as drugs such as heroin and ecstasy, clinical studies in the United States have been basically totally obstructed. The DEA states that:
Schedule I drugs [such as Marijuana], substances, or chemicals are defined as drugs with no currently accepted medical use and a high potential for abuse. Schedule I drugs [such as Marijuana] are the most dangerous drugs of all the drug schedules with potentially severe psychological or physical dependence. Some examples of Schedule I drugs are: heroin, lysergic acid diethylamide (LSD), marijuana (cannabis), 3,4-methylenedioxymethamphetamine (ecstasy), methaqualone, and peyote.
Regardless of your view on the validity of Marijuana’s current DEA scheduling, the results are clear. Limited access to marijuana for research purposes and few quality studies have directly shaped public option. Because there is almost no quality research available, most of the public view on marijuana has to be from anecdotal and lower quality sources. Someone who is trying to critically appraise the benefits and negatives of using marijuana is forced to turn to personal experience, experience of others or case reports. All of these sources of information are highly subjective and results are difficult to replicate and are therefore generally unreliable.
What Do We Know?
We know that Marijuana is the most commonly used illicit substance in the U.S and around the world. We know that two states (Washington and Colorado) have legalized recreational use and other states have passed laws legalizing medial use and/or decriminalizing recreational use.
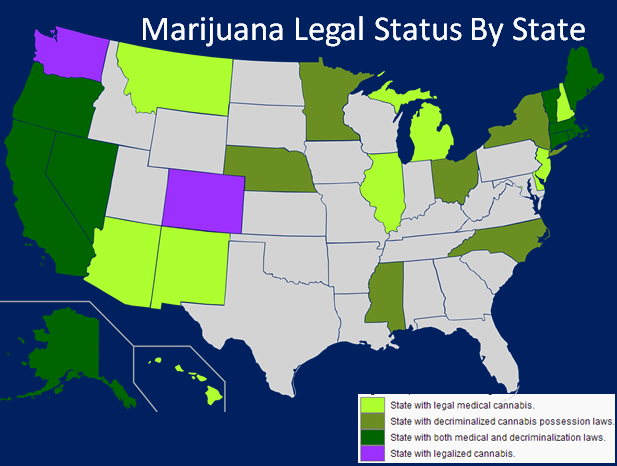 |
| Source: Wikipedia, accurate as of date of publication 6/6/14 |
The Federal Government has gone as far as to state that they will respect and not intervene in the states that have passed legalization laws. (1) Additionally, a bill has cleared the House and is currently headed to the Senate that would leave Medical Marijuana law up to the States. (2) We also know that Marijuana is less addictive than other illicit substances, but the fact that significantly more people use Marijuana leads to it having the highest prevalence of addiction of any illicit drug. (3)
What Do We Not Know?
What we do not know are the results of goal-standard, randomized controlled multicenter trials. We do not have these results because these types of studies do not currently exist. There are sporadic studies, of varying quality, many coming out of Israel, that attempt to help us better understand the impacts and possible medical benefits of smoking Marijuana. However, overall, there remains a lack of quality research.
How Can Quality of Life Research help us to Understand Marijuana’s Impact on Users?
Quality of Life research is utilized across medical specialties. It is promoted by the World Health Organization (WHO) because it is patient-centered, facilitates screening of at risk populations and can improve clinical outcomes.
As I mentioned in a previous post, QoL is a multidimensional construct that primarily concerns an individual’s personal evaluation of his or her life with regard to global health, handicaps or impairments, and daily living activities. QoL research helps us to better understand how someone interacts with the world around them and their satisfaction with social, educational, and occupational functioning. In the case of Marijuana, this data can help to explore sub-clinical impacts and differentiate outcomes in those who use Marijuana and those who do not.
What Does the Quality of Life Research Tell us About Marijuana?
Some of the highlights from the 9 studies that have utilized QoL measures in those who smoke Marijuana include: (Reference number of the cited study is included here, see reference list below.)
1. Chronic and daily smokers reported more anxiety and depression. They also report worse mental and physical QoL. (4,5)
2. The areas that were significantly worse in those who used marijuana include: Well-being, Satisfaction with life, Happiness, Needs fulfillment, Satisfaction with relations and Satisfaction with life’s potential. (5)
3. Some studies found that mental QoL was negatively associated with Marijuana use while physical QoL was not. (6, 7, 8)
4. The low mental QoL scores were reflected in Marijuana users reporting more emotional and physical problems that interfered with social activities and their ability to accomplish tasks. Regular users also reported feeling calm and peaceful less often and down-hearted and depressed more often. (8)
5. Individuals who consistently abstained from marijuana use or smoked very infrequently fared significantly better than those who smoked Marijuana on a regular basis. (4, 5, 6, 7, 8, 9)
6. Some studies found that as compared to regular or heavy users, occasional users did not report lower QoL scores. (4, 8, 9)
7. Women reported a larger negative impact on their QoL than men in several studies. This led to the conclusion that women who occasionally use Marijuana, unlike men who occasionally use Marijuana, have worse QoL than non-users. (7, 8)
8. One study of HIV patients who used Marijuana found that the QoL of subjects who reported marijuana use did not differ from subjects who reported not using Marijuana. (10).
9. There are no randomized controlled trials that include QoL measures in populations of Marijuana users. All of the studies are cross-sectional or cohort studies. These studies are limited to finding associations between variables. The studies can find that two things are more or less likely to exist together. However, only randomized controlled trials can establish if one thing directly causes another to happen. In regards to the marijuana research, therefore, the studies available cannot distinguish the directionality of the relationship between Marijuana and QoL. They can and did establish, in all but one study, that low QoL is more common in those who regularly use Marijuana. However, they cannot distinguish whether Marijuana causes lower QoL or if lower QoL leads them to smoke Marijuana.
10. There was one open label trial (subjects knew if they were getting Marijuana or placebo) of 13 marijuana users. Patients were provided with prepared cigarettes each month. There was no standardization of dose of active Tetrahydrocannabinol (THC) or strain of Marijuana. THC is the substance in Marijuana that leads user to experience many effects including feeling “high.” Patients were instructed to take up to 3 inhalations per use, whenever they felt pain. With this being the best prospective clinical trial, you get a sense of how much we do not know, because quality research has been so limited. (11)
11. When compared to other drugs of abuse including alcohol, methamphetamine, heroin etc Marijuana’s association with worse QoL was much less than these other illicit substances. The other drugs of abuse were 6-20% more detrimental to QoL than Marijuana. The other substances also had a consistent negative association with Physical QoL, whereas Marijuana did not. (5, 6, 10)
12. One study looked at quitting Marijuana and found that stopping use did not improve QoL significantly. (12)
Is This Research Game Changing?
Overall, reviewing these 9 research studies did not change my view very much about Marijuana and the recommendations I give my patients. QoL research is designed to look at the patient as a whole. It can determine how a person is impacted by external factors and how a change in their environment or health changes the way they view the world around them.
Looking at the research as a whole, there is clearly a trend that heavy and chronic marijuana use is negatively associated with QoL. This means that heavy users generally report worse QoL than non or occasional users. The negative association is stronger in women. The findings from these studies makes me concerned that regardless of the purpose of the Marijuana use, recreational or medical, users seem to have a worse mental outlook than non-users. As a psychiatrist, this is particularly troubling.
After reviewing this data and other available research, I still feel that there is not enough quality clinical research to support the use of medical Marijuana for any specific purpose. I am aware that there are many anecdotal stories of personal accounts of Marijuana being used to stop seizures, treat glaucoma and cancer, and improve factors like appetite and sleep. However, until there are randomized clinical studies that look at the risks, benefits and alternatives to Marijuana, for treatment of these specific diseases and conditions, I cannot responsibly consent my patient for treatment. Every other medication currently available to my patients has gone through these same trials and FDA approval prior to reaching the marketplace. Let me be clear, no one doubts that propofol can help you sleep or that amphetamines can give you energy, however, no doctor is going to recommend that use you either of them for these purposes, because of the risk of side effects and because the safety concerns are too large.
The questions of side effects and safety profile remain for Marijuana because it has not been fully tested against placebo controls. We just do not have the data, at this point, for me to safely recommend and support its use for any medicinal purposes. I hope we get the research, because the anecdotal stories are very powerful. They are strong enough to change CNN commentator and neuro-surgeon Dr. Sanjay Gupta’s view. He is now supporting Marijuana utilization for medical treatment after a long history of opposition. He cites many individual and unique success stories, and not clinical research studies, for changing his position. Click here, to read his latest thoughts. I am optimistic that the research will come, and will guide our interventions. However, I think as a physician, we must stay evidence-based, consistent with our standards of a peer reviewed process and unfortunately the body of research just is not there yet.
What Does This Research Mean to Me?
I have some recommendations if you use Marijuana recreationally, for medical purposes, or are thinking about using. The answers are complicated and not “one size fits all.” There are several factors to consider when deciding if Marijuana is right for you and in predicting how Marijuana will affect you:
A) Marijuana factors: The potency and the makeup of the active cannabinoids differ depending on the strain you are using. Cancannabidiol (CBD) is the 2nd most commonly found cannabinoid and has the opposite effects, in many cases, when compared to tetrahydrocannabinol (THC). Therefore, users must be aware that no two strains of Marijuana are exactly alike. Additionally, trying to generalize the effects of Marijuana as a whole is overly simplistic. (13)That would be like comparing the effects of all mushrooms. We know mushrooms range from edible to poisonous. Marijuana strains nearly have as wide a range of effects on users. Therefore, we must look at the effects and the makeup of specific Marijuana strains. Over generalization of the global effects of Marijuana is one of the major limitations of the studies I reviewed above. None of these studies differentiated what strain of Marijuana was used and therefore worked under the likely false assumption that all Marijuana strains have the same effects on QoL.
 |
| These price tags show the THC and CBD contents of the Marijuana. |
B) Patient factors: The age, sex (men vs women) and comorbid/co-ocurring diagnosis(s) of the user all impact the effects of Marijuana. The above studies point out that women who occasionally use Marijuana report lower QoL, while men who use occasionally do not. There are likely many other differences between young and old users and men and women. Their is growing evidence that Marijuana may have a negative impact on adolescent’s brain development and lead to lower IQ scores later in life. Click here, to read the full NIDA report that was release today. Other diseases and conditions also likely impact the effects that Marijuana, like any drug, has on a user.
C) Dosing Factors: The modality of use (smoking, vaporizing, eating), Quantity (high vs low) and frequency of use (daily, weekly) all influenced the findings in the above studies. Take these factors into consideration as you decide whether Marijuana is right for you. More frequent and chronic users reported lower QoL than occasional users in the above studies for example.
Concluding Thoughts
Overall, I hope these studies and my commentary have helped you to better understand the research that is available and how we can use it to shape our understanding of Marijuana. Whether Marijuana is more or less dangerous than alcohol, or if it should be legalized nationally for recreational use, are separate discussions entirely. My goal with this post was to discuss the current evidence that supports the medical use of Marijuana. If you are using Marijuana recreationally you can use the data and discussion presented here to better understand the effects that Marijuana may have on you. QoL research is designed to explore effects that are sub-clinical, or in other words, less obvious than the physical changes that are oftentimes more apparent. As I continue to critically evaluate the research, my opinions and recommendations will remain fluid. If Marijuana really has medicinal properties, the research will come out and support it.
The views I have stated here should in no way serve in the place of a formal consultation with your doctor or suggest anything but following of Federal, State and local laws. We are expecting a lot of new data out of Washington State and Colorado and this will hopefully open the door to increased research on the Federal level as well. I will continue to follow the data and use it to guide my recommendations and clinical practice.
I look forward to hearing your thoughts and any research you feel is relevant to the discussion!
Best,
Dr. Goldenberg
docgoldenberg@gmail.com
docgoldenberg.com